Seeking Help, Finding Hope
Mental Health Challenges and Solutions for Asian Americans in New York City
REPORT MATERIALS
Introduction
Asian Americans are one of the fastest-growing populations in the US and in New York State and City, but they have been largely ignored by the mental health system. They tend to use mental health services less often than other groups, which leads to a lack of research on their mental health needs and challenges.1 This can create a false impression that Asian Americans do not need or want therapeutic support.2 However, the recent surge of hate crimes, racism, and violence against Asian Americans during the COVID-19 pandemic has exposed the hidden and unaddressed struggles they face, and the significant mental health stressors that affect this diverse community.
This report by the Asian American Federation (AAF) aims to address the gaps in research on the challenges to getting mental health care by gathering feedback from Asian Americans in New York City. AAF created surveys in 10 languages and collaborated with 15 partner organizations that serve Asian New Yorkers. We collected 543 surveys from Asian New Yorkers of 23 unique ethnic backgrounds.
In addition to holding AAF’s focus group session in English, our partners facilitated similar sessions in Bengali, Hindi, Korean, and Mandarin. Participants in the focus groups were invited to share their opinions, experiences, and challenges related to mental health for themselves and their communities. Our partner organizations recruited the survey respondents and focus group participants, in all cases except for AAF’s own English focus group.
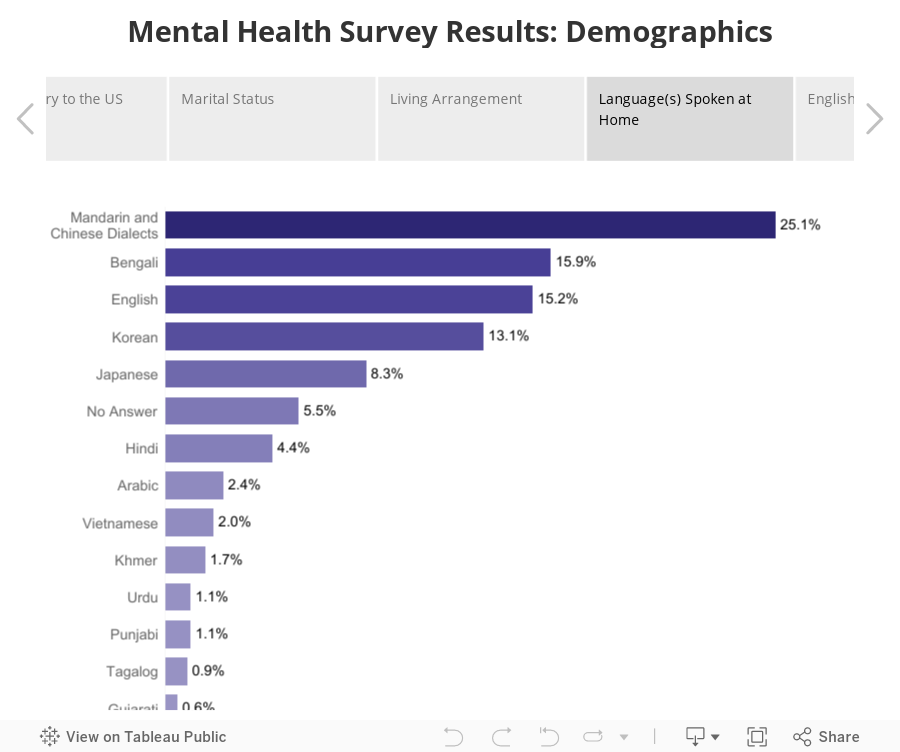
Of those who reported their ethnicity, we received the most survey responses from people who self-identified as Chinese (29%), Korean (16%), Bangladeshi (14%), Japanese (11%), Indian (7%), and Filipino (7%). Of those who responded, the most common languages spoken at home were Chinese (25%), Bengali (16%), English (15%), Korean (13%), Japanese (8%), and Hindi (2%). The majority of survey respondents were between 25 to 49 years old (34%), followed by those 65 years and older (26%). Almost two-thirds (63%) identified as female. A little over half of respondents were naturalized citizens (52%), and just under a third were non-citizens (32%). While this study does not use random sampling, the analysis in this report serves as a resource about mental health in Asian American communities specifically in New York City, including views from different ethnic groups, age groups, and citizenship status. The people who shared their responses and views here are connected to community organizations that serve various Asian ethnic groups. However, the situation may be worse for those who do not seek community support. For more comprehensive details, please refer to the Methodology Section.
The Issues that Affect Asian American Mental Health

The term “Asian American” covers a diverse group of people from different Asian countries, languages, cultures, and religious traditions. They also exhibit a wide disparity in income levels, and this gap has expanded more than in other major racial or ethnic groups in recent years. The mental health struggles that affect one Asian community are not identical to another: They vary from the trauma of war survivors from Laos, Cambodia, and Vietnam; to the memories of Japanese Americans in internment camps during World War II; to the stress of reconciling their cultural identity with American life for the children of first-generation immigrants.
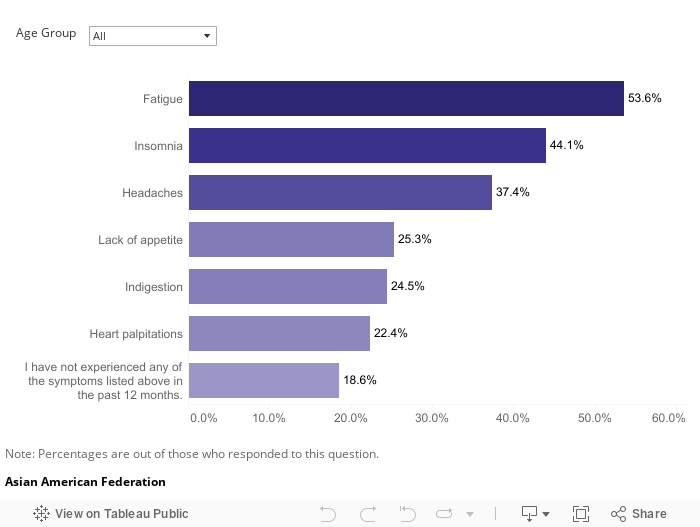
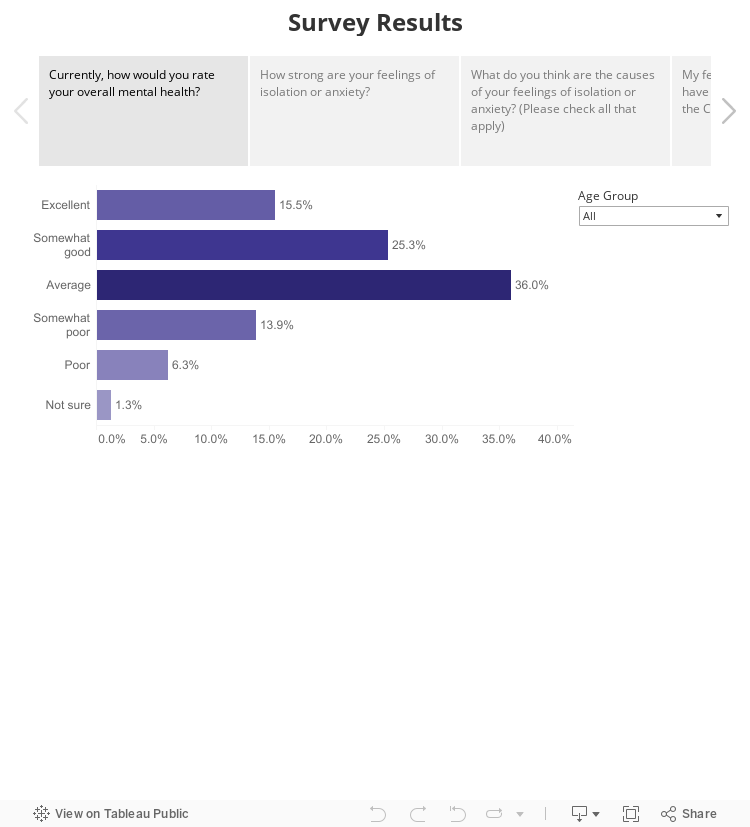
Roughly 65% of survey participants indicated that they experience feelings of isolation or anxiety to some extent, with almost 40% describing these emotions as “somewhat strong” or “very strong.” The majority of survey respondents reported consistently experiencing at least one of the symptoms outlined in Chart 1 over the past 12 months, and 45% indicated that they require assistance with their mental health issues.
Chart 1
In the past 12 months, have you PERSISTENTLY experienced ANY of the symptoms listed below? (Please check all that apply)
While more disaggregation of data on the mental health issues among different ethnic, age, or socioeconomic groups within the communities is needed to provide a fuller picture as to the unique challenges faced by different communities, the survey and focus groups that we conducted shed light on some systemic challenges affecting the mental health of Asian Americans as a whole.
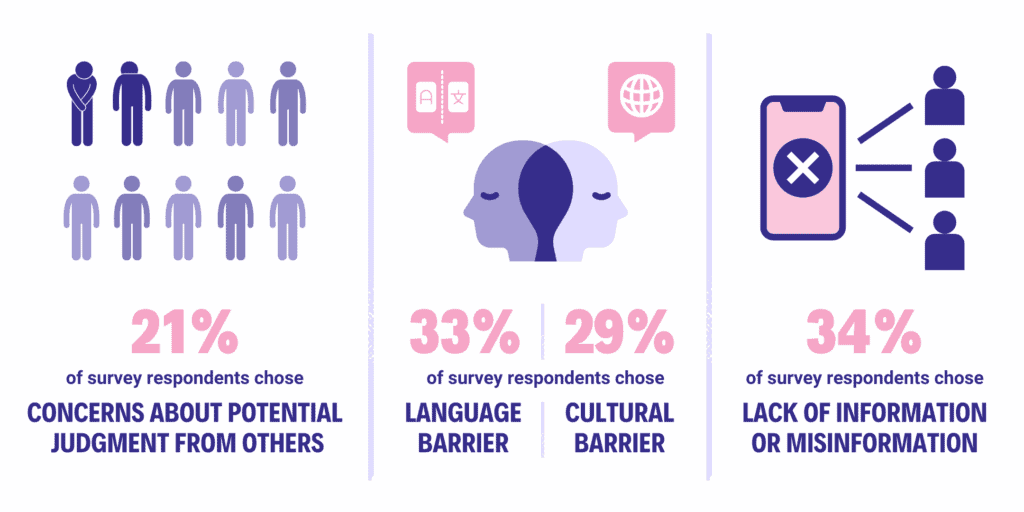
Figure 1
Primary Factors Contributing to Mental Health Challenges Among Asian Americans in New York City
For Many the High Cost of Living in New York City Adds to Mental Stress
The high cost of living in New York City poses substantial challenges for Asian Americans, dispelling the misconception of universal financial prosperity within this community. Nearly one-third of the Asian American population in New York City are low-income, a fact that contradicts the false belief that they are all wealthy and successful.3 Living in New York City is very expensive, and the everyday struggle to make ends meet can have a damaging impact on their mental well-being.
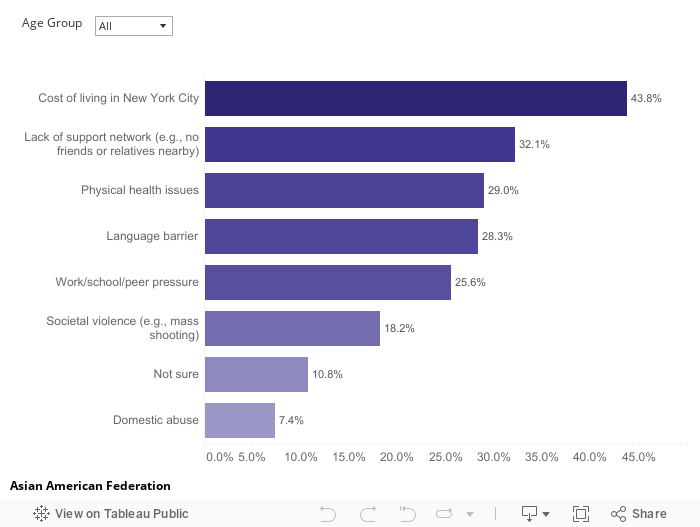
Survey findings show that nearly 44% of respondents cited New York City’s high cost of living as the top reason for their feelings of isolation or anxiety (Chart 2). The struggle to meet these high living expenses leads to chronic financial stress and anxiety, particularly for those with limited resources. This persistent financial strain can either trigger new mental health issues or worsen existing ones.
“It’s true that, in New York, we spend around 73% of our income on housing. After paying for rent and utilities, I am almost out of money… Prices are spiking every day, and rent and cost for my children’s education are also increasing, so all that affects our mental health.”
– Immigrant woman of Bengali origin
More critically, the high cost of living may deter individuals from seeking professional mental health support. Nearly one-quarter, or 24%, of survey participants reported that cost is the primary reason that they are not seeking mental health services (Chart 4). The urgent need to meet pressing financial obligations often takes priority over one’s own well-being. This hesitancy can result in delayed or overlooked mental health care, potentially worsening existing mental health conditions.
Seeking mental health care can be delayed or overlooked altogether, which can worsen their mental health issues. It is even harder for new Asian immigrants or those with language barriers. The complex healthcare and insurance system, as well as the lack of affordable and suitable mental health care, pose extra difficulties for them. Their mental health needs are further aggravated by the high costs and language barriers that prevent them from accessing vital support.
Chart 2
What do you think are the causes of your feelings of isolation or anxiety?
The “Model Minority” Myth and the Pressure to Succeed
The “model minority” stereotype imposes a burden on Asian American communities, perpetuating a widespread and misleading belief that portrays them as uniformly well-adjusted. This stereotype suggests that they achieve greater socioeconomic success than other minority groups through a strong work ethic, conformity to social norms, and academic excellence. The focus group participants suggested that those who have internalized the model minority myth may feel additional pressure to succeed. This pressure can, in turn, affect mental health and well-being, leading individuals to experience imposter syndrome or feelings of shame and guilt as they grapple with the fear of letting others down.4
According to our surveys, about a quarter of survey respondents who were familiar with the model minority myth felt that it had a negative impact on them. For example, the model minority myth is especially damaging to those who do not fit the stereotype, particularly the image of Asians excelling in academic spaces.
“I feel like because I wasn’t able to fill the myth of being smart in every subject, that I wasn’t good enough or I wasn’t performing high enough.”
– Chinese American adoptee in her early 20s
Growing up in a culture that often places a strong emphasis on family and collectivism, Asian Americans also may feel a responsibility to do well, enabling them to help the family financially or otherwise move forward. Oftentimes, they worry about being able to “pay back” their families for the sacrifices their families have made. An example is feeling anxiety over being able to find a job that pays enough to help the extended family.
“[I]f you don’t succeed, you have nothing else; you have to be the one that succeeds. So it puts a lot of pressure [on me].”
– Chinese American in their early 30s
Being Seen as the “Perpetual Foreigner” is Damaging to the Psyche
The perpetual foreigner stereotype is a damaging and misguided belief imposed on individuals who deviate from the perceived notion of a “typical” American, often due to their appearance, ethnicity, or language proficiency. This stereotype is notably pervasive in the media’s treatment of Asian American communities, where nearly half of the population in New York City grapples with limited English proficiency. This language barrier not only hinders effective communication, often leading to misunderstandings or misinterpretations, but it also fosters presumptions about one’s nationality, cultural heritage, and, ultimately, their rightful place in the United States.
Even for later generations of Asian Americans who are fluent in English, this stereotype wrongly assumes that individuals of Asian descent are foreign-born or struggle with English. Questions like “Where are you really from?” and comments like “You speak English so well” perpetuate this stereotype. These microaggressions – subtle yet hurtful interactions that Asian Americans might encounter daily – further exacerbate feelings of isolation and loneliness, as they are continually seen as outsiders based on their race.
“Microaggressions are really meant to make people feel like lesser human beings. There’s another term for microaggressions: Death by a thousand cuts. I think that description really does speak to the cumulative effects.”5
– Dr. Warren Ng, director of clinical services for the Division of Child and
Adolescent Psychiatry at New York-Presbyterian Morgan Stanley Children’s Hospital
Racial and Religious Intolerance Affects Mental Wellbeing

The historical legacy of racial and religious intolerance in the U.S. has deeply affected Asian American communities, leading to widespread implications for individual mental health and overall well-being. Individuals may struggle to find a sense of belonging in a society that may not fully accept or understand them and therefore suffer from profound feelings of isolation and loneliness. In some cases, individuals may choose to withdraw from social interactions altogether as a means of self-protection. For example, Asian American children and adolescents have faced bullying in educational settings due to stereotypes about their facial features or other physical attributes. This form of discrimination has led to feelings of inadequacy, self-doubt, and even trauma, with long-lasting effects on their mental and emotional well-being.
Religious minorities within the Asian American community, such as Muslims and Sikhs, face unique forms of discrimination. They are often targeted for their religious attire, such as turbans or hijabs. Another particularly troubling manifestation of racial and religious intolerance is the assumption of criminal status of Muslims due to Islamophobia.6 This unjust and unfounded presumption can have serious consequences, leading to unfair treatment, harassment, and even violence. The constant threat of discrimination can lead to a state of hypervigilance, where individuals are constantly on guard, anticipating potential instances of prejudice. This state of heightened awareness can be mentally exhausting and emotionally draining.
It is important to recognize that Asian Americans may experience discrimination based on multiple intersecting identities, such as race, religion, gender, and/or sexual orientation. These compounded forms of discrimination can create complex and layered mental health challenges for individuals and communities.
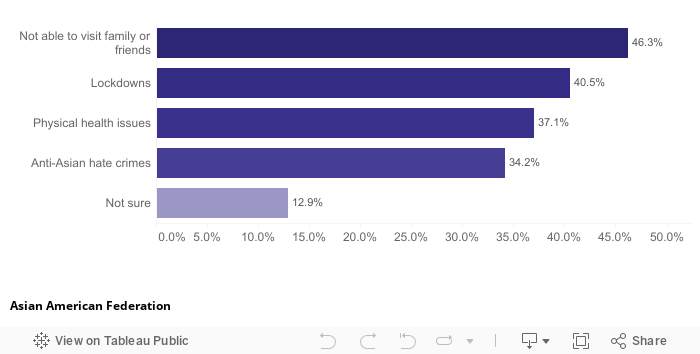
COVID-19 and the Loss of Safety and Security
The COVID-19 pandemic, with its social distancing measures and lockdowns, heightened feelings of isolation and loneliness for many. This, in turn, has amplified experiences of anxiety and depression. Based on the survey results, over half of the participants reported that their feelings of isolation or anxiety had gotten worse since the pandemic. And almost half of respondents marked a reason for increased feelings of isolation or anxiety as not being able to visit family or friends (Chart 3).
“I couldn’t go outside for the past three years…I was very worried. I couldn’t go visit relatives, either. You could pass on the virus to one another. I had so many worries. I have felt depressed for three years.”
– Immigrant senior of Chinese origin
Asian Americans have faced a dual impact on their mental health due to the sensational reporting and labeling of the “China Virus,” particularly in the early stages of the pandemic. This rhetoric has unfairly stigmatized and held Asians responsible for the virus’s spread. Consequently, this climate of fear increased anti-Asian sentiment, resulting in a surge of hate crimes, xenophobia, and discrimination. Witnessing and imagining their loved ones, especially the elderly and vulnerable, becoming victims of these senseless acts has caused a great deal of secondary trauma for Asian Americans. Many are reliving past experiences of personal trauma or discrimination that they had previously pushed aside.
For numerous individuals, there has been a profound loss of a sense of safety and security. The fear of venturing out and engaging in normal activities has not only restricted their freedom but has also limited their capacity to find joy and lead the life they desire. Among those who reported that their feelings of isolation or anxiety had gotten worse since the pandemic, 34% identified anti-Asian hate crimes as the main cause (Chart 3).
Chart 3
Why do you think your feelings of isolation or anxiety have intensified since the start of the COVID-19 pandemic?
Asian Americans Struggle to Get Quality Mental Health Care
Asian Americans are less likely to receive mental health treatment compared to other racial/ethnic groups, with only 20.8% of Asian adults with mental illness receiving treatment in 2020.7 This disparity is due to various systemic barriers in accessing mental health care and quality treatment, further intensified by stigma and the absence of culturally appropriate and integrated care. These challenges can lead to exacerbated symptoms and a deterioration in the quality of life when treatment is either unavailable or delayed.
Figure 2
Barriers to Accessing Mental Health Services
Cultural Attitudes including Shame, Stigma and Denial also Discourage Help-Seeking
Over 21% of survey respondents cited concerns about potential judgment from others as the main reason for not seeking treatment for their mental health needs (Chart 4). In Asian American communities, mental health issues are often associated with the fear of “going crazy,” or losing control over one’s mind. Regrettably, mental health struggles can be viewed as sources of shame or disgrace within these communities, capable of potentially tarnishing the family’s reputation. Seeking support for such challenges is stigmatized, seen as an admission of personal or familial failure, leading to a loss of face in the community. This powerful stigma acts as a significant barrier, discouraging individuals and their families from seeking the help they may desperately need. As a result, many delay seeking assistance until a crisis emerges, perpetuating a harmful cycle of stigma and reluctance to seek help. This cycle persists because preventive measures are not implemented to avert these crises in the first place.
“I knew I was sick, [but] I was afraid to go to the doctor. I was afraid of being laughed at, I was afraid of people being like, you know, you’re a psychopath or you’re mentally ill or whatever. So I avoided going to see a psychiatrist [in] Flushing [because I live in Flushing]. That’s why I went to [see a psychiatrist in] Brooklyn, because I was afraid of being laughed at, because of your self-esteem, because you’re afraid of being humiliated.”
– Immigrant woman of Chinese origin
“This is like an ugly thing in the family. You don’t talk about ugly things in the family to outsiders. This is the main idea. It is almost like people don’t admit they have psychological problems.”
– Immigrant senior of Chinese origin
Older Asian Americans have often lived through periods marked by severe economic hardship or human rights abuses. These difficult circumstances have contributed to the development of a culture characterized by resilience and self-reliance. As a result, there is a tendency to downplay or dismiss mental health challenges as less important compared to more immediate, tangible hardships. Moreover, there’s a prevailing cultural belief that one should rely on inner strength to navigate such challenges without seeking external support. Against this cultural backdrop, Asian Americans, particularly those who are younger, feel pressured to navigate mental health issues on their own, without burdening others, possibly making their struggles worse.
“[It’s] really difficult for people who grew up in these communities to express themselves because it’s…like, our parents did it. They were able to struggle this much, and they succeed[ed]. Why shouldn’t we be able to do that, too? Do we really need to go to therapy, or are we just being kind of soft?”
– Indian American in his mid 20s
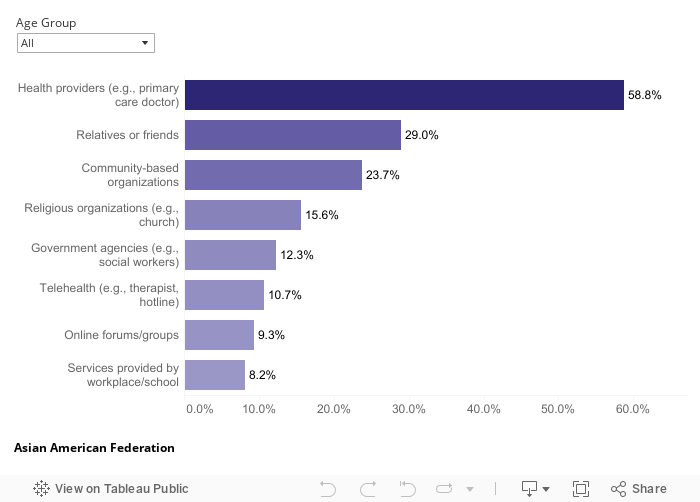
Faith and spirituality have important influences on mental health, especially within Asian American communities marked by notable religious diversity. In contrast to the U.S. average, a higher proportion of individuals in these communities identify as Buddhist, Hindu, Muslim or adherents of other spiritual affiliations.8 Faith communities often offer a built-in social support system. In our survey, 16% of respondents selected religious institutions as their chosen source for mental health support. (Chart 5). However, religious communities may perpetuate stigma around mental illness that can delay professional treatment. For example, some Asian cultures characterize mental illness as divine punishment, bad karma, disturbed flow of life energy, or imbalance of basic elements inside the body, or even possession by evil spirits.9
Chart 4
Which of the barriers listed below, if any, make it hard for you to access mental health services?
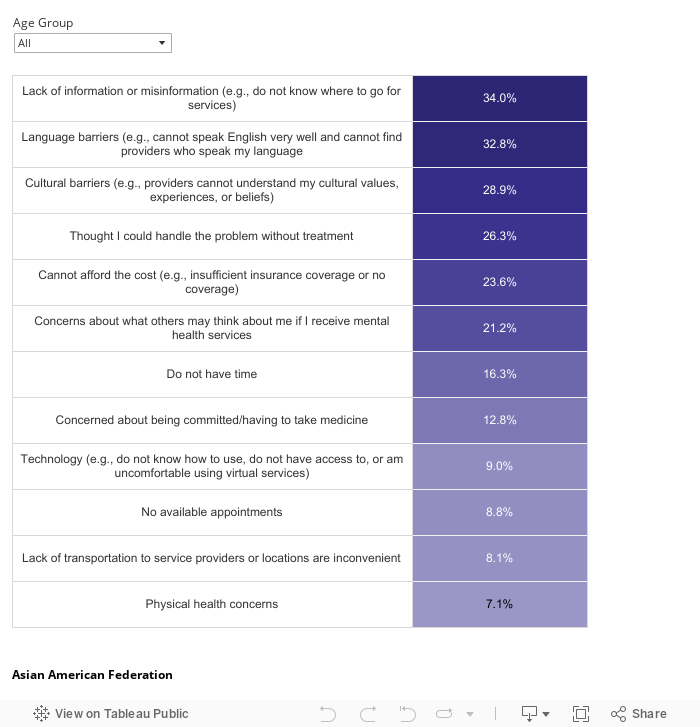
Chart 5
In general, where do you go if you need mental health services or support?
Language Barriers and Lack of Culturally Competent Programs Present Significant Challenges
The growth of the Asian American population in New York City is mainly driven by immigration, resulting in a significant number of Asian Americans who do not speak English as their primary language. Almost half of Asian Americans in New York City have limited English proficiency, and this rate varies widely depending on nation of origin. Additionally, 72% of Asian Americans aged 65 years and older have limited English proficiency.
Thus, language barriers and limited availability of culturally appropriate mental health service providers may prevent people from getting the care they need.10 Based on the survey results, language barriers (e.g., cannot speak English very well and cannot find providers who speak my language) and cultural barriers (e.g., providers cannot understand my cultural values, experiences, or beliefs) were reported as two of the top three barriers that prevent people from accessing mental health services (Chart 4).

“[My grandmother] needed someone who spoke a certain dialect [of Chinese] that is not Cantonese or Mandarin. And that made it exponentially more difficult to find a mental health provider who spoke that particular dialect. Members of my family had to play translator. And I don’t think she was happy about that. She couldn’t be ‘completely transparent’ with the provider for that reason. And because everything was going through a lens, I don’t think she felt as though she was getting the unfiltered real information.”
– Chinese American in his late 30s
Even when patients speak English proficiently, communicating about mental health can still be hindered by language and cultural barriers. Participants in focus groups expressed that the finer points of their mental health experiences were often overlooked when discussing them with someone who could not fully grasp their linguistic or cultural intricacies. For first-generation immigrants who have not yet mastered English, this underscores the necessity for mental health services in their native language. As for later generations who are fluent in English, it highlights the need for services attuned to their experience of straddling multiple cultures — a unique set of challenges related to identity, belonging, and acceptance.
“It’s starting with my name – you know what I mean? It’s kind of complicated in that way, and that’s one small way. [Therapists] just don’t even know how to wrap their heads around what being Asian or Asian American even means. [I] shared nothing in common [with my old therapist]. So whatever upbringing that I was having, whatever I was telling her, she was putting it through her lens, and it just didn’t seem to click. So I think I did try to look for somebody whom you don’t have to explain your whole story to, right?”
– Chinese American student in his late 30s
The pandemic presented an added layer of difficulty for Asian New Yorkers with limited English proficiency, owing to language and cultural barriers. As crucial information was predominantly disseminated in English, individuals facing language difficulties encountered challenges in accessing essential resources, comprehending public health guidelines, and securing appropriate medical care. This gave rise to feelings of isolation and uncertainty, particularly as they grappled with pivotal decisions concerning their health and safety.
Furthermore, Western mental health services employ approaches that may feel unfamiliar to Asian immigrant patients. Providers in Western contexts often rely on open and intimate conversations about sensitive and emotional topics for diagnosis and treatment. This can potentially clash with Asian cultural values, which traditionally steer away from public discussions of such matters to maintain face and preserve personal dignity. The disparity in communication styles can create a significant barrier for individuals seeking mental health support within the Western healthcare framework.
“We can’t speak English properly, we can’t speak like Americans; how they speak and how we speak creates a disconnection, we couldn’t explain properly.”
– Immigrant senior of Bengali origin
Limited Mental Health Literacy and Preference for Alternative Treatment Philosophies
Mental health literacy refers to the “knowledge and beliefs surrounding the recognition, management, and prevention of mental health illnesses.”11 Seeking mental health treatment and services first requires recognizing the features of mental illness, which, in many Asian cultures, is a concept that simply does not exist. Instead, mental health issues may be more readily perceived by their physical manifestations among the Asian community, such as feeling extreme fatigue, headaches, stomachaches, or other symptoms. Over 80% of survey participants consistently reported experiencing one or more physical symptoms in the past 12 months, such as fatigue, insomnia, and headaches. However, only 45% of these respondents expressed a desire for mental health support. This discrepancy suggests that Asian Americans may be more comfortable addressing physical ailments than acknowledging and seeking help for mental health issues.
The limited mental health literacy in Asian American communities has also created a substantial void in accessing critical information about mental health support. According to survey respondents, the foremost barrier that hinders access to reliable mental health resources is the lack of information or the presence of misinformation (e.g., not knowing where to go for services) (Chart 4). This dearth of accurate guidance leaves many individuals feeling lost and unsure of how to address their mental health needs. In response to this uncertainty, some Asian Americans, particularly first-generation immigrants, gravitate towards traditional or non-Western forms of medicine as their primary mode of treatment, rather than considering it as a complementary approach. This reliance on traditional or alternative healing methods can be attributed to a lack of familiarity with Western mental health services and a preference for approaches deeply rooted in their cultural heritage. These practices, which often emphasize the integration of mind and body in maintaining health and promoting healing, include, but are not limited to:12
- Traditional Chinese medicine
- Ayurveda – the traditional medicine of India
- Kampo – Japanese herbal medicine
- gSo-ba Rigpa – Tibetan medicine
- Acupuncture
- Massage therapy
- Folk nutritional therapy
- Energy healing exercises (e.g., tai chi, qi gong)
- Guided meditation
- Spiritual healing
However, while these practices hold cultural significance and value, this cultural inclination for familiar therapies could potentially cause delays or reluctance to pursue mental health care, even for serious mental health conditions.
“I don’t think we have that much information about this in our community on how to help people. I always see violence and Asian hate in newspapers and death. But I don’t see any programs for us to take care of mental health issues.”
– Cantonese-speaking immigrant senior
Recommendations
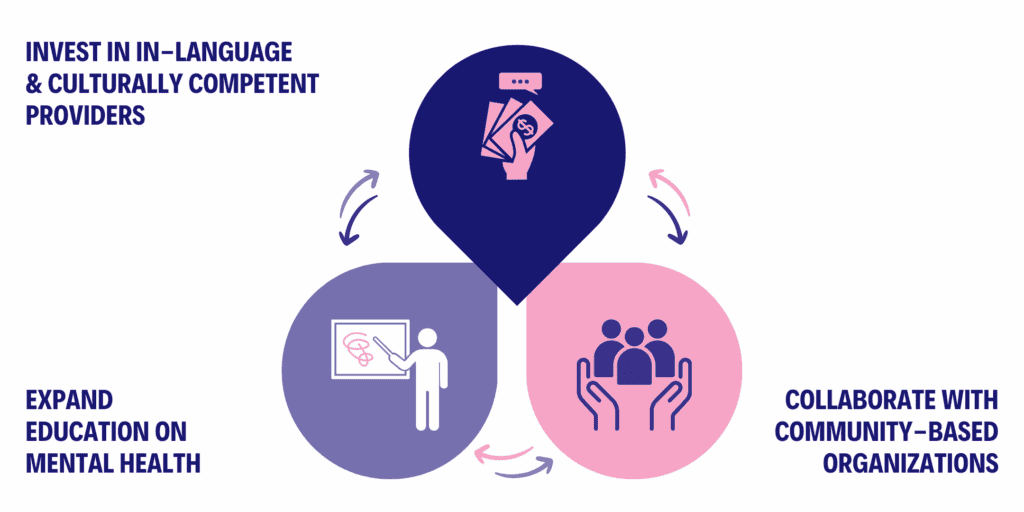
While we acknowledge the broader need to make mental health services more affordable and reduce the difficulty of exploring insurance options, this section concentrates on specific recommendations tailored to the distinct challenges that Asian American communities experience, including expanding mental health education, investing in in-language and culturally competent providers, and partnering with community-based organizations.
Figure 3
Quality and Accessible Mental Health Services for Asian American Communities
Expand Mental Health Education
Many Asian Americans do not seek help for mental illness in the first place because they lack knowledge about the causes of, and treatment for, mental illness (see the section on Limited Mental Health Literacy). Educational programs and materials that are culturally relevant to the experiences and values of Asian Americans and raise awareness about mental health, as well as cover common mental health conditions, their symptoms, and available support resources, can dismantle the stigma around mental health. They should also be distributed through the channels that Asian Americans already use to get mental health information (Chart 6).
Normalize Seeking Help
It is important that educational programs and materials are geared to help people recognize that mental illness is a legitimate health issue, similar to conditions like asthma and diabetes, with effective treatments available. They must encourage the notion that seeking help for mental health concerns is a demonstration of strength, not a sign of weakness.
“If you’re somewhat health-conscious, you might see your primary care doctors because you think you might be at risk for diabetes. It’s not because you’re sick, but more about taking steps to prevent serious illnesses in the future, right? The connection is pretty clear when it comes to physical health. But for mental health, it’s different. I think people, especially in Asian communities, often wait until things are really bad, to the point where they can’t hide it anymore. By the time they reach out for help, it’s often quite late. There’s a lot more work needed to make it normal to seek help early on, before things escalate to such a point.”
– Dr. Jihan Ryu, Psychiatrist at Hamilton Madison House
Share Personal Narratives to Break Stigma
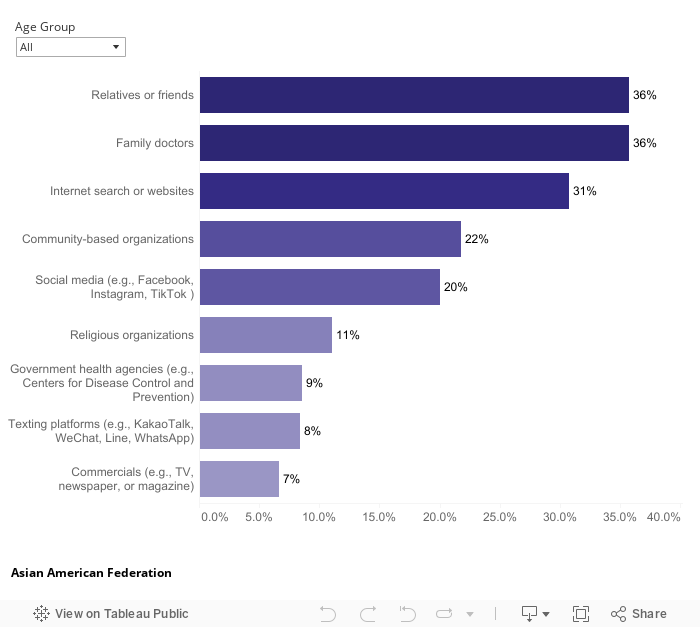
The survey results reveal that friends and relatives are the most sought-after source for mental health information among participants (Chart 6). Thus, sharing personal stories of how community members navigated mental health challenges and recovered can make discussions about mental health more commonplace and acceptable.
Collaborate with Physical Health Care Providers
Over a third, or 36%, of survey participants indicated that they would turn to family doctors as their preferred source for mental health information (Chart 6). Therefore, it is critical to forge partnerships with physical health care providers, including primary care physicians and specialists, to integrate mental health discussions into routine check-ups and medical appointments.
Chart 6
Where do you go for mental health information?
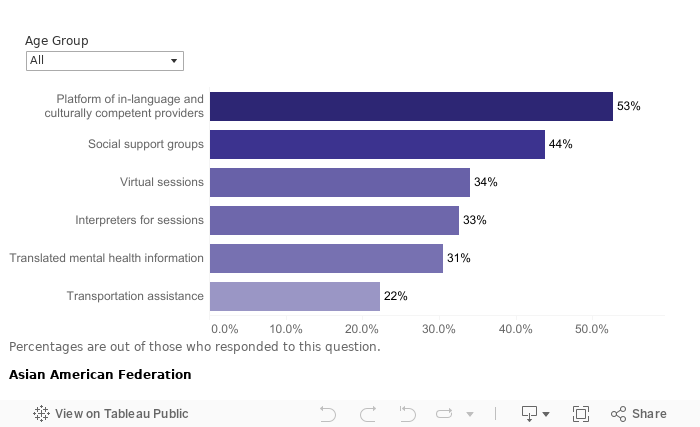
Invest in In-Language and Culturally Competent Providers
Over half, or 53% of survey respondents, expressed a preference for platforms that feature in-language and culturally competent providers as their primary choice for overcoming barriers to accessing mental health care (Chart 7). For example, AAF launched an online Mental Health Directory that features hundreds of providers who collectively speak over 17 Asian languages. The directory is part of AAF’s efforts to help Asian New Yorkers find culturally relevant mental health help and find providers to fit their needs, whether that means counseling, education, or other diverse ways that Asian communities use to seek mental well-being.
While there are more Asian Americans working in the mental health field than before, we still need greater numbers to more accurately reflect the rapid demographic changes taking place in the state, city and country.13 Developing job opportunities and recruiting students to study mental health should be a priority for fast-growing communities, as they urgently need a workforce geared to meet their specific and growing needs. Federal funds can use scholarships and loan forgiveness to support the professional education of these students, while grants to schools, organizations, and/or agencies can help create jobs and programs that promote their personal, academic, and professional well-being. Grants may also be used to train diverse peer specialists (individuals who have experienced mental health challenges themselves and provide support to those in need) from within local Asian American communities. Mental health professionals should try to be more aware of their own implicit bias and judgments. This includes Asian American mental health professionals who may also harbor and internalize their own racism and judgments.
Nonetheless, research shows that ethnic matching (pairing a client with a therapist on race/ethnicity alone) is not always effective, which is understandable.14 Rather, culturally-attuned providers who are mindful of cultural factors and family expectations are key to overcoming barriers.
“Just because you’re Asian, or just because you’re Chinese doesn’t mean that you will be the best therapist for Chinese people. We all have our own assumptions and biases. Being able to speak the language does not automatically make you a good psychiatrist. Keep an open mind and stay curious, and remember, sometimes we’ve got to dig a little deeper to really figure out how to help someone out.
I also think we need to get culturally competent care happening not just one-on-one, but in groups and throughout the whole system. We should feel it’s totally okay for providers to ask their patients or coworkers things like, ‘I don’t really know much about this part of your culture, but I’m eager to learn and understand it better.’ You know, making it feel safe and open for those kinds of conversations.”
– Dr. Jihan Ryu, Psychiatrist at Hamilton Madison House
Chart 7
What specific services do you want more to address these barriers?
Be Sensitive to Asian Family Dynamics
Asian family dynamics emphasize a strong connection between the individual and the family unit, which can be at odds with Western ideals of patient autonomy and privacy. As a result, navigating these cultural differences can be complex.
In some cases, it may be uncomfortable or inappropriate for family members to share confidential information. However, involving adult children and/or other caregivers in discussions about treatment can benefit some patients in different settings. Furthermore, Asian families often make decisions collectively, which means that they may want to involve the whole family in the treatment plan. In order to do so, they would need to navigate hierarchical roles and relationships. For example, this may mean any of the following: the whole family must be on board with the treatment plan; those in traditional gender roles may feel uncomfortable speaking about mental health issues and require a “go-between” or proxy to communicate their feelings; and these families may appreciate different visitor or after-hour policies.
Be Attuned to an Implicit Communication Style
It is important to note that some Asian American individuals may not feel comfortable using direct verbal communication, as it may be viewed as impolite or harsh in certain Asian cultures. It is important for mental health providers to be attuned to implicit and nonverbal communication cues conveyed by certain Asian American clients, instead of expecting communication to be direct, explicit, and/or demonstrative, which can happen when providers lack cultural humility.
For example, older generations in the Asian American community may, consciously or not, express mental distress through physical symptoms due to cultural beliefs and stigma. Therefore, it is often more acceptable to talk about feeling tired or experiencing physical discomfort than to directly express emotional distress. Inquiring about sleep patterns or appetite can serve as a constructive starting point for conversation.
“They may believe that it’s not acceptable to say, ‘I feel sad,’ but it’s OK if I say, ‘I’m very tired and my bones hurt.’ It’s not acceptable to be anxious and say, ‘I’m worried.’ But it might be OK if I say, ‘I’m feeling shaky.’ There’s more of a cultural acceptance of the physical manifestations of mental illness.”
– Dr. Nadine Chang, a clinical psychologist and chair of the Asian Psychiatry
Program at Gracie Square Hospital, which is affiliated with NewYork-Presbyterian15
Offer an Action-Oriented Approach
Action-oriented interventions—such as behavioral activation, which focuses more on changing behavior—can be helpful for Asian American clients, along with other interventions. They can include tracking daily activity to understand how mood fluctuates with different tasks and then identifying meaningful activities to do each week, especially those that are enjoyable or rewarding.
This pragmatic approach for Asian Americans can shift the focus away from individual mental illness to an external problem that can be solved. By steering clear of instilling a sense of shame, therapists can help clients to develop problem-solving skills for external challenges, which then “could be an avenue into more traditional approaches in which there is a focus on thoughts and feelings.”16
Case Study
Adopting a Holistic Approach to Mental Well-Being: Asian Bicultural Mental Health Services at Henry Street Settlement
At the Community Consultation Center (CCC), Henry Street Settlement recognizes the growing mental health needs of the Asian immigrant population. Since 1997, their Asian Bicultural Mental Health Service has been a part of the Outpatient Mental Health Clinic at CCC, offering culturally attuned outreach, diagnosis, and treatment services in Cantonese and Mandarin.
Their services address the stigma related to mental illness within Asian families; social and economic stressors; and family conflicts in values and role expectations that often arise between the older and younger generations in a new culture. They also connect participants to a network of programs, ranging from a food pantry; to ESOL classes; to job readiness and training; to social groups, which allow them to succeed beyond the walls of the CCC.
The Case of “Y”
Counseling has played a pivotal role in Y’s life, enabling her to overcome daunting challenges and secure meaningful employment. Born in China, Y, now 29, moved to the U.S. when she was 14. She came to Henry Street’s Community Consultation Center in 2015 after a hospital discharge—one of nearly a dozen over the years. Adjusting to life in the U.S. had proved immensely challenging for Y, exacerbated by the tragic loss of her brother and her battle with paranoid schizophrenia. Isolated, with no support system outside of her family, Y felt neglected due to traditional gender preferences favoring her brother and a lack of understanding among those around her that her illness was not just a sign of weakness.
Through culturally sensitive counseling, Y has come to understand that it is okay to seek help. Engaging in support groups and weekly one-on-one therapy sessions, she has become better at managing her condition, and her self-esteem has improved. The support she received over the years bolstered her confidence, allowing her to secure a part- time job as a home health aide. Additionally, counseling empowered her to embrace educational opportunities, including ESOL classes at Henry Street. Y’s determination, supported by counseling, has led to new friendships, greater financial security, and, most significantly, more than a year without a hospital admission.
Collaborate with Community-Based Organizations
Community-based organizations that directly serve Asian American communities possess an in-depth understanding of the cultural norms, values, and beliefs prevalent within those communities. They can bridge the gap between traditional cultural practices and modern mental health approaches. Equipped with staff and/or volunteers who are fluent in various Asian languages, community-based organizations are trusted entities within their respective communities. Their established relationships with community members can help reduce the stigma associated with seeking mental health support. Charts 5 and 6 reveal that 22% of survey respondents prefer receiving mental health services at community-based organizations and 24% turn to these organizations for mental health information. With targeted funding, community-based organizations can play a pivotal role as “cultural brokers” for mental health services aimed at Asian American communities in the following ways:
Reduce Stigma and Increase Awareness
Proficient in effective communication styles, as well as the complex family structures and dynamics within Asian households, these organizations are well-positioned to conduct outreach and educational campaigns about mental health; disseminate information about mental health challenges in order to dispel cultural stigmas surrounding mental health; and promote a more accepting and open-minded perspective.
Serve as a Bridge Between Community Members and Mental Health Providers
Community-based organizations can serve as a hub for connecting individuals to a network of culturally competent mental health professionals, ensuring they receive appropriate care. These organizations can also offer training and workshops to mental health professionals to enhance their cultural competency so that providers are equipped to deliver effective and sensitive care to Asian American clients.
Fill Gaps in Providing Services
Lastly, community-based organizations can directly design and implement mental health programs and initiatives that align with the specific needs and preferences of the respective communities they serve. Nearly half, or 44%, of survey respondents highlighted the importance of support groups as crucial to breaking down barriers in accessing mental health services (Chart 7). Community-based organizations emerge as the primary choice for these groups, with their ability to offer thoughtfully designed physical and virtual spaces and create an atmosphere of trust, openness, and acceptance. Such spaces encourage individuals to share their mental health concerns without fear of judgment or discrimination. And, in contrast to the clinical approach, community-based organizations frequently offer more imaginative platforms for expression, incorporating art therapy or creative writing, often in culturally sensitive ways.
“Someone told me about Garden of Hope around 2007. I have come here to them, and it has become a habit. It’s that kind of feeling that others can’t understand. Now I feel like I’m getting better, and there are some things that are entirely healed, like taking medicine. After taking the medicine, you think very clearly and well.
I’ve started to reduce the usage since then, and I reduced it slowly, continued to meet with counselors at Garden of Hope, and then participated in some activities. Now I feel better because I’m getting older, but I still hope doing this kind of mental health counseling is actually pretty good. I like it.”
– Garden of Hope focus group participant
“Due to the COVID-19 pandemic, getting a mental health counselor appointment was not so easy. I had to search a lot, and my insurance was not sufficient to cover the expenses. In this situation, I contacted Sapna NYC, where they offer me all services for free.”
– Immigrant of Bengali origin
Case Study
Enhancing Access to Mental Health Services: The CONNECT Program

The Continuous Engagement between Community and Clinic Treatment (CONNECT) program is a vital component of the behavioral health services provided by Hamilton-Madison House. This program is dedicated to enhancing access to mental health services for the pan-Asian American community in the Lower East Side, particularly in the Two Bridges/Chinatown area.
The CONNECT program, staffed by a skilled team of case managers, prescribers, psychiatrists, nurses, and three licensed clinicians fluent in Mandarin, provides a range of services including psychiatric assessments and education; psychotherapy; medication management; group treatment; and referrals to clinical programs. Recognizing the importance of easy communication and cultural understanding, CONNECT is also expanding its language services to include clinicians who speak dialects like Fuzhounese and Shanghainese, ensuring that more clients can converse with their providers and receive culturally competent care.
To combat stigma faced by Asian American communities, CONNECT uses innovative strategies to create a supportive, welcoming environment for those seeking help. The program assigns each client a dedicated psychiatrist and clinician in order to build a personalized support system. With flexible scheduling, ranging from daily to less frequent sessions, it adapts to clients’ changing needs. They also offer psychotherapy in unconventional settings like homes, parks, or cafes, fostering trust and ease, especially for hesitant clients. Clients can also choose to stay in Hamilton-Madison House’s clinical program, ensuring continuous, tailored mental health support.
The program stresses the importance of family support during treatment. By inviting family members to join sessions and providing them with resources for caregiver stress, the program not only strengthens the support for clients but also significantly increases the likelihood of continued services. Family involvement is crucial for emotional support and reinforces the client’s commitment to seeking and maintaining mental health care.
Recognizing the importance of community for personal well-being, especially with increased social isolation after COVID-19, the program has started to offer activities like dance and calligraphy classes in order to strengthen community bonds and reduce isolation. These efforts not only help individuals feel connected but also build a stronger, supportive community focused on mental health.
Methodology
AAF designed the surveys and focus groups to understand the mental health needs and challenges of the Asian American communities in New York City. A number of AAF’s member and partner agencies collaborated in conducting these surveys and focus groups. All data provided to AAF for analysis was anonymized prior to submission.
Survey
Fourteen of AAF’s member and partner agencies took part in the survey. These agencies include the Arab American Association of New York (AAANY), Asian Americans for Equality (AAFE), Council of Peoples Organization (COPO), Garden of Hope (GOH), Hamilton-Madison House (HMH), Homecrest Community Services (HCS), India Home, Japanese American Social Services, Inc. (JASSI), Korean American Family Service Center (KAFSC), Korean Community Services of Metropolitan New York (KCS), Mekong NYC, National Federation of Filipino American Associations (NaFFAA), South Asian Council for Social Services (SACSS), and Sapna NYC.
The survey employed a convenience sampling design, targeting Asian American adults who were receiving services from these member and partner agencies. The sample was stratified by demographic characteristics such as gender, age, and English proficiency to capture a diverse group of non-institutionalized Asian Americans aged 18 and above, residing in New York City. For gender, each organization was instructed to have a sample representing roughly 50% of females and 50% of males. For age, the sample should include at least two from the following age groups: young adults (18-35 years), middle age (36-55 years), and older adults (56 years and older). Whenever possible, we requested that 30% of the sample should be from the older adults group who are among the more vulnerable members of the community. And to reflect the community accurately, the sample should include at least 50% respondents who have limited English proficiency (LEP). More specifically, each organization targeted a particular language group with varying sample sizes, depending on their respective capacities (see Chart 1). Between March 31, 2023 and May 31, 2023, 543 Asian adults from 23 different Asian ethnic groups participated in in-person surveys. All participants received $20 as incentive.
Table 1
Survey Samples
| Organization | Targeted Language Group | Targeted Sample Size | Responses Collected |
| AAANY | Arabic | 20 | 20 |
| AAFE | Chinese (Mandarin/Cantonese) | 40 | 40 |
| COPO | Urdu | 30 | 30 |
| GOH | Chinese (Mandarin/Cantonese) | 40 | 40 |
| HMH | Chinese (Mandarin/Cantonese) | 40 | 40 |
| HCS | Chinese (Mandarin/Cantonese) | 40 | 43 |
| India Home | Bengali | 30 | 39 |
| Hindi | 10 | ||
| JASSI | Japanese | 40 | 60 |
| KAFSC | Korean | 40 | 41 |
| KCS | Korean | 40 | 49 |
| Mekong | Khmer | 10 | 20 |
| Vietnamese | 10 | ||
| NaFFAA | Tagalog | 30 | 40 |
| SACSS | Bengali | 10 | 39 |
| Hindi | 30 | ||
| Sapna | Bengali | 40 | 42 |
The surveys were developed in English and translated into Arabic, Bengali, Chinese (Simplified and Traditional), Hindi, Japanese, Khmer, Korean, Tagalog, Urdu, and Vietnamese. Surveys were available in both paper and digital (Google Forms) formats. All the organizations had staff or volunteers who spoke Asian languages on site when respondents filled out the survey. They briefly introduced the purpose of the survey; informed the respondents that by completing the survey they were consenting to participate in the evaluation study; and helped respondents go through the questions without skipping any that applied to them. Before being submitted to AAF for analysis, all survey responses in Asian languages were translated into English.
Focus Groups
Between July 18, 2023 and August 31, 2023 AAF and its member and partner agencies—AAFE, GOH, HMH, India Home, KAFSC, and Sapna—conducted six in-person focus groups in total. These groups recruited 46 adult participants representing 4 distinct Asian ethnic groups across New York City. Each organization had specific criteria for recruiting participants, including considerations for gender, age, and language, tailored to the population they serve (see Chart 2).
Table 2
Focus Groups Recruitment Criteria
| Organization | Targeted Language Group | Age Group | Gender Breakdown |
| AAF | English | 18-30 | 50% Male and 50% Female |
| GOH | Mandarin | 18+ | 100% Female |
| HMH | Mandarin | 50+ | 50% Male and 50% Female |
| India Home | Bengali | 50+ | 50% Male and 50% Female |
| KAFSC | Korean | 25-50 | 50% Male and 50% Female |
| Sapna | Bengali | 18-25 | 50% Male and 50% Female |
Recruitment took place concurrently with the survey process (as described earlier), wherein respondents were informed that those meeting the focus group criteria and expressing interest could share their contact details. From these respondents, eight eligible participants were identified. They confirmed their availability for the focus group and completed an informed consent form. To account for potential no-shows, organizations recruited additional participants. On average, about five participants attended each focus group session. Every attendee was offered an $100 incentive for their participation. The focus group sessions were two hours long, beginning with a 15-minute segment for introductions and initial questions, followed by the main discussion, and concluding with a 5-minute debriefing at the end.
AAF created a moderator guide for the focus group sessions, which was translated into Bengali, Chinese, Hindi, and Korean. Except for the focus group conducted by AAF in English, all the other focus group sessions were conducted in Asian languages, with native language speakers serving as moderators. Before fielding any focus groups, moderators attended a training conducted by the New York Academy of Medicine on the moderator guides and the overall research objectives of the study. For in-language sessions, the conversations among focus group participants were video recorded, transcribed, and translated into English. These transcriptions were then forwarded to AAF for analysis.
